
Recovery from Stroke

The Physio for Seniors Rehabilitation Team has helped many seniors recovering from stroke. Each case outcome is very different, from almost complete patient recovery to significant changes required in the level of patient care. In every case, a rehabilitation treatment plan is key to regaining any physical function lost.
CASE STUDY:
Patient N.N. suffered a left Cardiovascular Accident (CVA), or stroke, which caused right-side weakness.
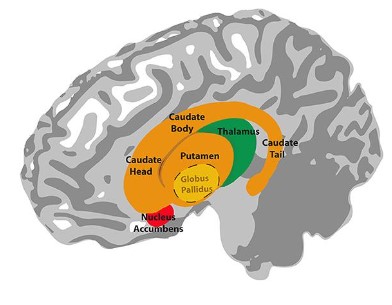
Basal Ganglia Hemorrhage:
Patient N.N. experienced a CVA that was caused by a burst blood vessel in the basal ganglia tissue of the brain. Blood filled the area and cut off oxygen and glucose nutrition to the caudate nucleus, putamen and globus pallidus.
A hemorrhagic stroke in the basal ganglia causes these specific symptoms:
Changes in Movement
- Ataxia: a lack of voluntary coordination of muscle movements that includes ABNORMAL GAIT
- Stiff, rigid muscles
- Loss of movement due to muscle weakness
- Tremors
- Weakness in muscles used for swallowing, talking or smiling
Cognitive Impairment
- Loss of ability to make decisions
- Memory loss and attention deficit
- Language difficulties
These deficits can improve with time, but rarely do they return to pre-stroke functioning. N.N. and his family receive information, education and support from a variety of healthcare professionals such as Physiotherapists, Occupational Therapists, Counselors. Learning compensatory strategies and techniques is a large part of the treatment plan to achieve the Outcome Measure set for N.N.
Personality Changes
- Change in judgment
- Confusion and difficulty understanding what is happening
- Frustration, anger and anxiety
- Can become unmotivated or exhibit a lack of interest in activities once enjoyed
- Inappropriate emotional responses (may cry or laugh for no apparent reason)
- May suffer from depression(Livestrong, 2011)
It is estimated that 30-60% of patients have depression after CVA. (Martin, 2007, p.292)
Patient N.N’s GOAL: To walk again and to be able to perform Activities of Daily Living such as dressing himself and taking a shower.
Presentation at start of Rehabilitation: Poor standing posture – bent at the knees, torso is forward and his gaze is downward. He is cautious and reports feeling weak. He requires support (1 person assisting to stand at the bar and holds on with both hands). N.N. has shown signs of confusion during sessions and needs short, clear verbal and visual instructions to be able to participate in exercises. Although he has reported feeling down, he is very motivated to work hard to achieve his recovery goal.
Nick worked on strengthening, correcting posture and improving balance in sit to stands with his Physiotherapist.
Outcome Measure for N.N.: Patient will be able to ambulate 50 metres with a single point cane SAFELY and without assistance maintaining a healthy blood pressure reading consistently for 5 consecutive sessions so that he can function independently at home and at work by 30/04/2024
- Performance: walk 50 metres safely with a single point cane
- Criteria: no stopping to rest, no loss of balance for 5 consecutive Physiotherapy sessions while maintaining a healthy blood pressure.
- Condition: Independently
- Time frame: by 30/04/2024 (6 weeks from discharge from hospital)
Levels of Assistance Measure:
- Independent: Patient requires no assistance or cueing in any situation and is trusted in all situations 100% of the time to do tasks safely.
- Supervision: Caregiver/Physio is not required to provide any hands-on assistance but may need to give verbal cues for safety.
- Contact Guard/SBA: Caregiver/Physio must be on Stand-By Assist (within arm’s length for Patient’s safety.
- Minimum Assistance: Caregiver/Physio provides 25% physical and/or cueing assistance.
- Moderate Assistance: Caregiver/Physio assists Patient with 50% of the task. Physical assistance and/or cueing.
- Maximum Assistance: Caregiver/Physio assists Patient with 75% of the task. Physical/verbal cueing.
- Dependent: Patient is unable to assist in any part of the task. Caregiver/Physio must take weight of client during ambulation, guiding foot forward and cueing throughout ambulation (Early. p.180)
The Levels of Assistance Measure is useful because it is easy to understand by both the Rehab Team and family members who can use it to record N.N.’s progress. An important point to remember however is that patients with CVA can vary in ability from one day to the next. Progress can be up and down, it is therefore important to add a consistency measure to address variability. For example, Patient is independent to walk 50 metres with no assistance or cueing for 3 Consecutive Days.
The Physiotherapist will monitor:
Blood Pressure
Normal blood pressure is recognized as 120/80. N.N.’s blood pressure reads around 108/76 most days. This is fine. However, it is not uncommon for CVA patients to have fluctuations in blood pressure, especially during mobilization or exertion. Careful monitoring of BP is essential. If pallor, sweating, laboured breathing, disorientation, confusion or distress is observed then therapy stops to allow the patient to rest and recover. Heart and breathing rates are taken and recorded. A drink of water can help to elevate blood pressure to a safe level if it has dropped. If blood pressure is raised this can precipitate another stroke so regular vitals checks are done.
Red Flags!
- A drop in systolic pressure of more than 20mmHg or below pre-exercise level
- A rise in systolic pressure to greater than 200mmHg and diastolic pressure to greater than 110Hg is a warning sign to cease activity and seek medical advice from a nurse or doctor. (Safe Mob.)
Respiration Rate
Normal respiration is measured at between 12 and 16 breaths per minute. N.N.’s RR has been 18 bpm at rest. The physiotherapist will check his lungs regularly for the ability to clear secretions and to check if dysphasia has caused any aspiration of fluids into the lungs. If Blood oxygen saturation (SpO2) is less than 88% or there is any cyanosis (blueness in the skin around the nose and lips or extremities), if respirations are counted at <5 or >40 or if the Patient exhibits shortness of breath, he should not be mobilized. (Safe Mob.)
DVT – Deep Vein Thrombosis (blood clot)
DVTs can occur in people who have had a stroke or are at risk of stroke and N.N. has had one. Therefore therapists will monitor him for any changes in pain, swelling or shortness of breath that could indicate a clot issue. A good Physiotherapist will be in contact with their stroke Patient’s GP and/or nurse to share observations, progress and setbacks.
Outcome for N.N.:
Rehabilitation for N.N. has been slow and steady.
He has moved from Dependent to Moderate Assistance. Although the goal was to walk with a cane, he has found the use of a 4 wheeled walker easier. When ambulating with his 4ww he is at a Minimal Assistance Level. N.N. has been able to exercise with no fluctuations in BP and only mild shortness of breath as his endurance gradually improved. Posture is better with decreased flexion at knees, he is able to bring his torso back in line with the pelvis with verbal cueing and his gaze is now forward-facing. N.N. is able to walk 70 metres while maintaining healthy vitals and after one sit-down rest he is able to walk another 70 metres. Regular strengthening of the weak right side (both upper and lower extremity) has resulted in progressions in grip strength and resistance exercises increased to using 1lb weights. N.N. is able to dress himself on most days apart from donning compression socks for which he needs assistance. Showering is not yet independent and requires a caregiver assist but he is able to manage most of his personal hygiene well with minimal assistance. N.N tires more quickly than before his CVA and when he is tired he can become more irritable and confused, but with a good balance of therapy, rest and cognitive/emotional support from family and friends he is recovering.
Rehabilitation includes:
- Seated balance exercises
- Standing balance exercises
- Stretching muscles and soft tissues with particular focus on weak right side
- Strengthening and encouraging use of weak right side in functional movement exercises
- Massage for stiffness in muscles and soft tissues
- Deep breathing exercises
- Motivational support and encouragement
- Cognitive challenges while exercises